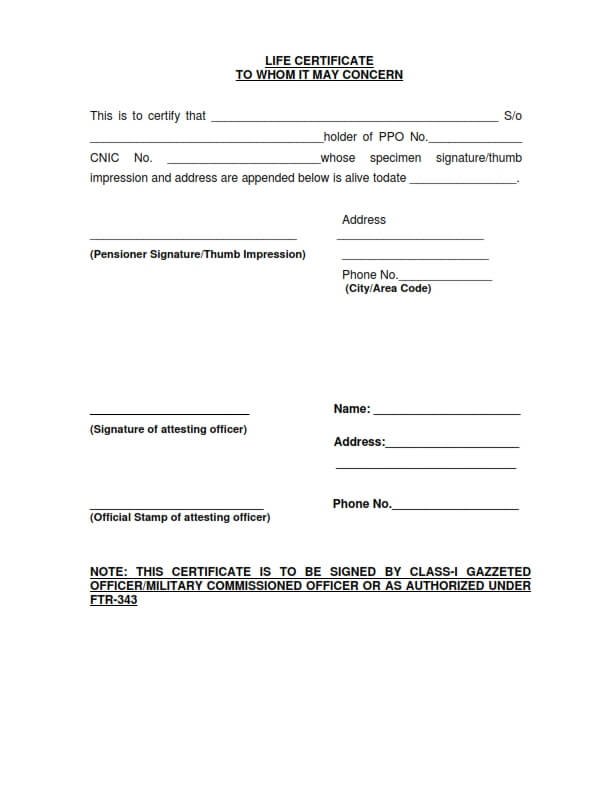
LIFE CERTIFICATE
TO WHOM IT MAY CONCERN
This is to certify that _______________________________ S/o _____________________________holder of PPO No.________ CNIC No. _________________whose specimen signature/thumb impression and address are appended below is alive todate __________.
Address: _______________________________________________________________
Phone No._____________________________________________________________
(City/Area Code) ______________________________________________________
(Pensioner Signature/Thumb Impression)
_____________________________________________________________________